Chest pain is a common complaint in emergency department (ED) patients. Patients with acute chest pain often present with concomitant symptoms such as dyspnea, diaphoresis, anxiety, nausea, or emesis.
While these additional symptoms can be helpful to the emergency provider (EP), caution should be taken when relying on any one symptom. Specifically, the association of anxiety or panic with a noncardiac cause of chest pain can be a risky assumption.
While some studies have shown a high prevalence of panic disorder within an ED chest pain population (as high as 20%), anxiety and panic itself are poorly specific findings.
Patients with acute life-threatening cardiac or pulmonary conditions frequently present with feelings of panic or impending doom in association with chest pain. This may even be in the setting of a stressful situation and mislead the EP to feel confident that anxiolytic therapy and reassurance is all that may be needed.
High stress and anger have been associated with an increased incidence of cardiovascular events
These stressful situations can be the catalyst for a more serious condition, as moments of high stress and anger have been associated with an increased incidence of cardiovascular events. These events are believed to occur from the catecholamine surge that is associated with acute emotional distress.
This can, in turn, lead to increased platelet aggregation and subsequent rupture of an unstable intracoronary plaque. Furthermore, multiple studies have shown a link between anxiety disorders and higher rates of cardiac risk factors. This suggests that patients with a psychiatric history may be at higher risk for cardiac disease.
Misdiagnosis of a cardiopulmonary condition as anxiety is a frequent occurrence
Unfortunately, misdiagnosis of a cardiopulmonary condition as anxiety is a frequent occurrence. A recent survey-style study of emergency medicine physicians found that nearly 10% of self-reported missed diagnoses consisted of acute coronary syndrome (ACS), pulmonary embolism (PE), or aortic dissection.
In addition to the patient consequences of a missed or delayed diagnosis, there are significant medicolegal implications as well. Roughly 7% of all malpractice claims for misdiagnosis are due to missed myocardial infarction (MI) or PE. With that in mind, EPs should undoubtedly think twice before excluding a life-threatening etiology of chest pain based primarily on the concomitant symptoms of anxiety or panic.
Takotsubo Cardiomyopathy – Condition Involving ACS and Emotional Distress
A less common, but well-described, condition involving ACS and emotional distress is takotsubo cardiomyopathy, also termed “broken-heart syndrome.” Patients with takotsubo often present with chest pain in the setting of recent emotional event (i.e., loss of a loved one).
Electrocardiogram (ECG) findings in patients with takotsubo can be similar to an acute anterior wall MI. These patients may even have elevations in cardiac biomarkers and echocardiogram findings that support a diagnosis of acute infarction.
Cardiac catheterization, however, reveals no culprit coronary lesions. Instead, dilatation of the left ventricle is seen with a pathognomonic appearance that resembles pots used by Japanese fisherman to catch octopi known as “takotsubo.”
While these patients typically undergo standard ACS treatment, ECG and ventricular function typically normalize within several months of the initial presentation. Importantly, the incidence of recurrence can be as high as 5% within 6 years.
Final Words
In general, while “anxiety” and “panic disorder” will likely remain frequent diagnoses for ED patients with chest pain, EPs must remain cautious to not prematurely jump to these diagnoses before a thorough evaluation is performed.
Key Points
- Misdiagnosis of a cardiopulmonary condition as anxiety is a frequent occurrence.
- Patients with acute life-threatening cardiac or pulmonary conditions often present with feelings of panic or impending doom in association with chest pain.
- Moments of high stress and anger have been associated with an increased incidence of cardiovascular events.
- Multiple studies have shown a link between anxiety disorders and higher rates of cardiac risk factors.
- Takotsubo cardiomyopathy is a reversible cardiomyopathy that occurs in the setting of a severe emotional event.
READ ALSO :
Suggested Readings
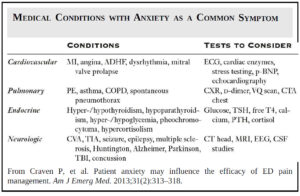
- Handberg E, Eastwood J, Eteiba W, et al. Clinical implications of the women’s ischemia syndrome evaluation: interrelationships between symptoms, psychosocial factors and cardiovascular outcomes. Womens Health (Lond Engl). 2013;9:479–490. https://pubmed.ncbi.nlm.nih.gov/24007253/
- Huffman J, Pollack M, Stern T. Panic disorder and chest pain: mechanisms, morbidity, and management. Prim Care Companion J Clin Psychiatry. 2002;4:54–62. https://www.psychiatrist.com/wp-content/uploads/2021/02/25294_panic-disorder-chest-pain-mechanisms-morbidity-management.pdf
- Mostofsky E, Penner EA, Mittleman MA, et al. Outbursts of anger as trigger of acute cardiovascular events: A systematic review and meta-analysis. Eur Heart J. 2014;35:1404–1410. https://academic.oup.com/eurheartj/article/35/21/1404/583173
- Schiff G, Hasan O, Kim S, et al. Diagnostic error in medicine, analysis of 583 physician-reported errors. Arch Intern Med. 2009;169:1881–1887. https://pubmed.ncbi.nlm.nih.gov/19901140/
- Sharma AK, Singh JP, Heist EK. Stress cardiomyopathy: diagnosis, pathophysiology, management, and prognosis. Crit Path Cardiol. 2011;10:142–147. https://journals.lww.com/critpathcardio/Abstract/2011/0900/Stress_Cardiomyopathy__Diagnosis,_Pathophysiology,.4.aspx