Table of Contents
What is Tumor Lysis Syndrome ?
- Tumor lysis syndrome (TLS) is a metabolic syndrome characterized by renal failure and multiple metabolic abnormalities caused by the rapid and massive cell destruction and release of intracellular content into the plasma.
- It typically occurs on rapidly aggressive hematologic malignancies or after treatment initiation in some solid tumors, such as high-grade lymphomas.
- TLS is probably one of the most common oncologic emergencies, with a spectrum of presentations ranging from minimally symptomatic to life threatening; its rapid recognition and treatment are essential for Emergency Physicians.
- The pathogenesis of TLS rests in the immense cell lysis after the initiation of therapy, commonly chemotherapy, although radiotherapy and steroids occasionally precipitate it as well.
- The syndrome is a combination of the electrolytic and inflammatory effects of the release of intracellular contents (potassium, phosphorus, and nucleic acids) as well as renal failure that follows secondary to crystal precipitation in the renal tubules, inflammatory mediator–driven vasoconstriction, and concomitant hypovolemia.
Operational Definition
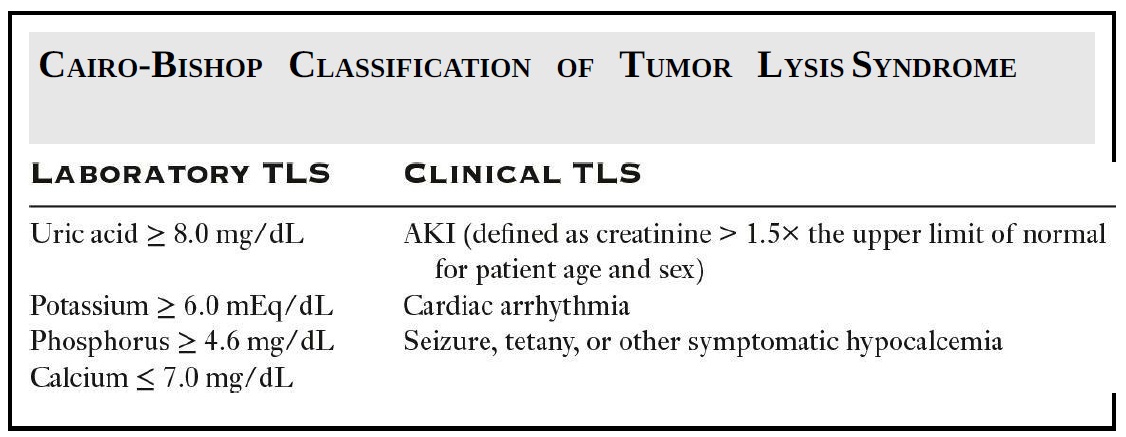
A universal definition of TLS has been difficult to achieve, and some controversy exists about the core characteristics of the syndrome. Currently, the Cairo and Bishop classification is accepted as the standard norm and distinguishes between laboratory and clinical TLS. In the regular emergency medicine practice, the distinction is not particularly helpful, but it is important to know it in order to have a cogent discussion with your nephrology or oncology consultant and to identify patients at risk of the disease who may benefit from close follow-up.
When to Suspect and How to Diagnose Tumor Lysis Syndrome
The symptoms of TLS are often nonspecific and when recognizable are related to hyperkalemia, hypovolemia, hypocalcemia, and renal failure. This syndrome is commonly underdiagnosed, and the major challenge is its identification; the diagnosis should be at least entertained in any patient with recent initiation of therapy for malignancy. A common mistake is to diagnose acute renal failure in these patients and move to treatment mode without looking into the cause.
Recognizing TLS is important as there is specific therapy that can make a difference. In others words, we need to overcome satisfaction bias and consider TLS as the etiology of new acute renal failure in oncologic patients. It is probably advisable to obtain a serum uric acid in all sick-appearing oncologic patients with new-onset renal failure.
Avoid Kidney Explosion
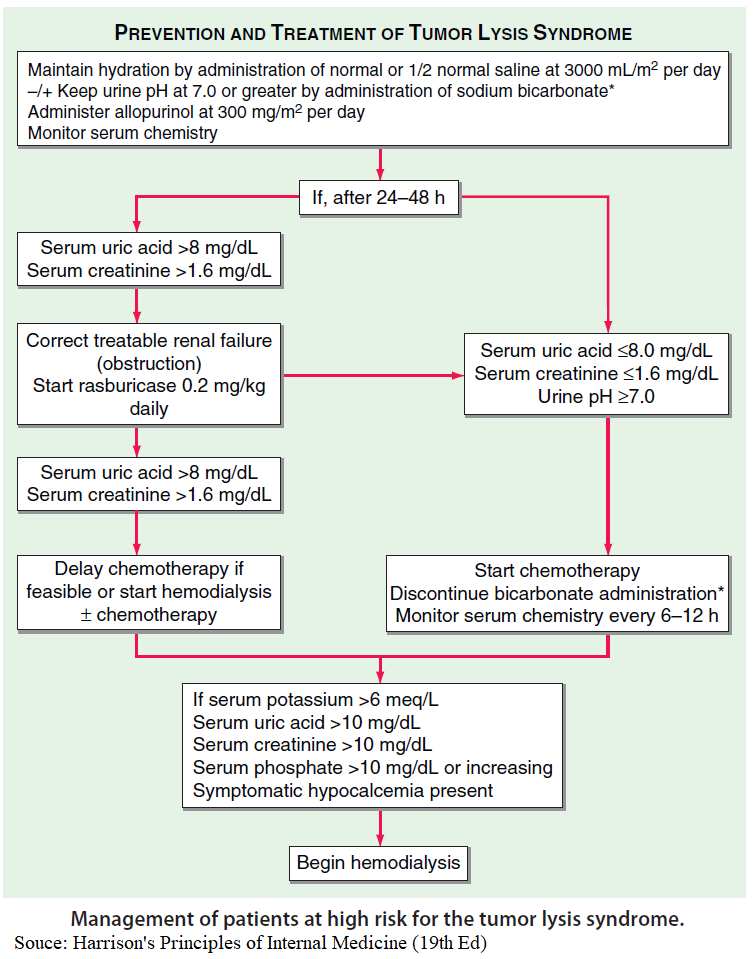
Although outside of the scope of control of emergency physicians, the prevention of TLS with pretreatment hydration and allopurinol is of paramount importance and a key detail in the clinical history to obtain.
- Patients who have mild clinical symptoms, are well appearing, and have normal or minimal renal dysfunction but developed chemical abnormalities should probably be admitted for hydration, allopurinol, and electrolyte monitoring.
- Patients with a similar clinical profile but with more laboratory abnormalities and signs of renal dysfunction should receive aggressive fluids, rasburicase, admission to an ICU, and consultation with oncology and nephrology.
The pharmacologic treatment of TLS is based on allopurinol and rasburicase.
- Allopurinol is a xanthine oxidase inhibitor that prevents the conversion of xanthines into uric acid; therefore it prevents the new uric acid formation but does not alter the acid already in the plasma.
- Rasburicase is a recombinant urate oxidase that converts uric acid into allantoin, making it more soluble and facilitating the excretion 5 to 10 times; the major issue is that the drug is very expensive and in some centers requires approval by oncology or nephrology before its use.
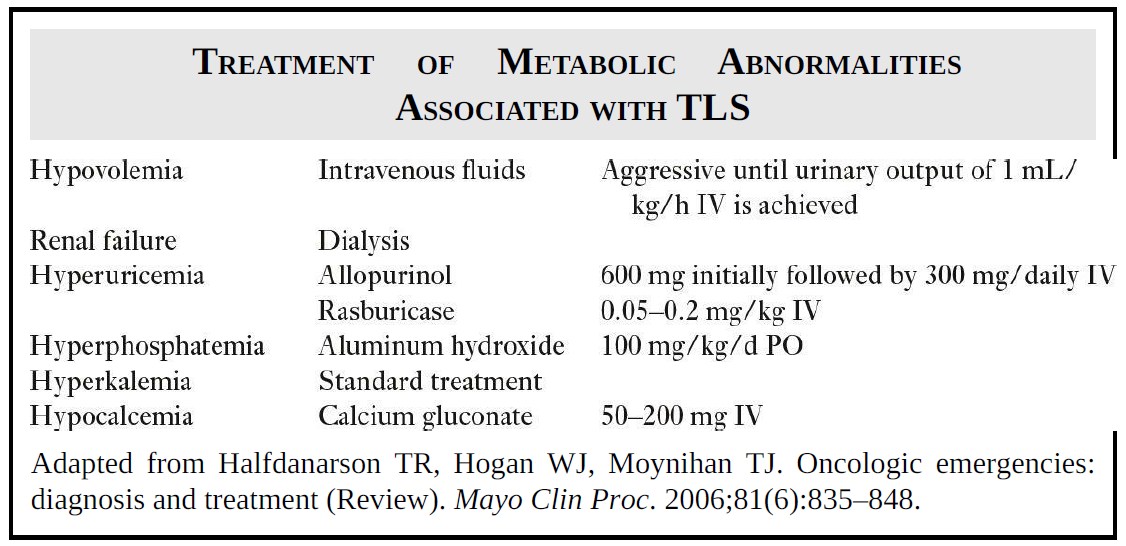
Treatment of Metabolic Abnormalities of Tumor Lysis Syndrome
The main problem is the patient with TLS who is clinically sick. Typically, these patients are extremely fragile, and management needs to be extremely precise, but at the same time, the overwhelming metabolic derangements can be, well, overwhelming.
The best way to approach this is to proceed into a step-by-step approach
- Contact nephrology as soon as possible as this patient may require hemodialysis soon.
- Start working on an ICU bed.
- Correct the hyperkalemia as soon as possible using your standard catastrophic hyperkalemia approach, but consider hemodialysis early.
- Correct hypovolemia in a septic shock–like aggressive fashion. Recommendations are 30 to 40 mL/kg until around 100 mL/h of urine output is achieved.
- Start allopurinol and ideally also use Rasburicase as it will inhibit the production of uric acid and will help to excrete already formed urates.
- Attempt to correct the hypocalcemia; however, this could be challenging and may require hemodialysis.
Hemodialysis in patients with TLS is frequent and usually is recommended more liberally compared to other renal emergencies; involving your emergency nephrologist early in the game is advisable. Among the indications of renal replacement are oligoanuria, volume overload, refractory hypocalcemia, and severe hyperkalemia.
Key Points
- TLS is more common than you may think in oncologic patients.
- Consider TLS in oncologic patients who are sick or with new renal failure.
- Aggressive fluids, allopurinol, and rasburicase are the main treatment.
- Don’t get overwhelmed by the magnitude of derangements; take care of the problems in order of lethality.
- Consider hemodialysis early.
![Read more about the article All About Leukemia: From Diagnosis to Treatment [A Comprehensive Overview]](https://manualofmedicine.com/wp-content/uploads/2023/04/Classification-of-Leukemias-According-to-Cell-Type-and-Lineage-300x213.png)