This post is an answer to the ECG Case 276
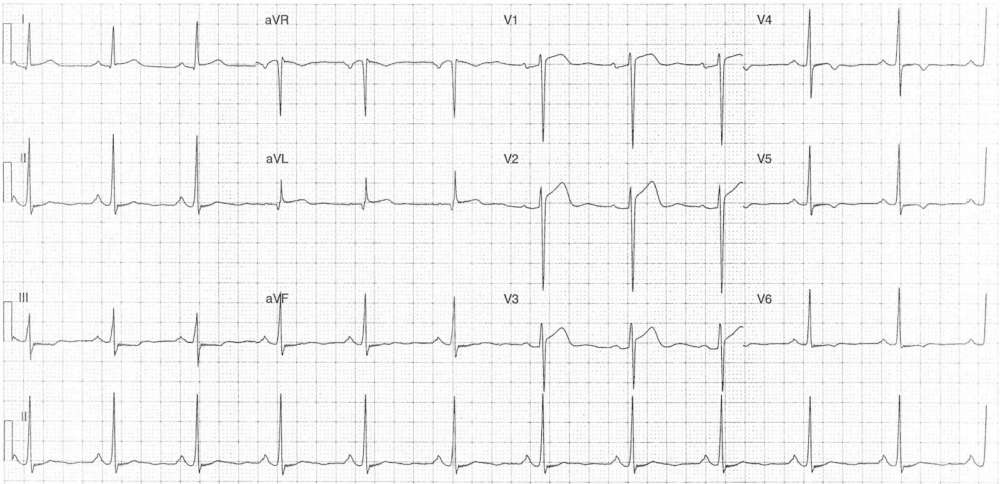
- Rate: 72 bpm
- Rhythm: Regular sinus rhythm
- Axis: Normal
- Intervals:
- PR – Normal (~180ms)
- QRS – Normal (80ms)
- QT – 320ms (QTc Bazette 380-400 ms)
- Segments:
- ST Elevation in leads I (0.5mm) aVL (0.5mm) V1 (2mm) V2 (3mm) V3 (2mm)
- Concave morphology
- ST Depression in III, aVF, V5-6
- ST Elevation in leads I (0.5mm) aVL (0.5mm) V1 (2mm) V2 (3mm) V3 (2mm)
- Additional:
- T wave inversion in leads III, V4-6
- Broad P wave in inferior leads with biphasic P wave in V1
- Left atrial abnormality (LAA)
- Voltage criteria LVH
- aVR ~14mm
- R wave V5 + S wave V1 ~35-36mm
- LV ‘Strain’ features – lateral ST depression and T wave inversion
Interpretation
LVH with secondary ST / T wave changes.
V3 suspicious for ACS given relative height of ST elevation in relation to R-S magnitude.
What happened next?
The patient had attended hospital ~2 years prior with chest pain and a similar ECG. At that time the patient was taken for urgent PCI which showed no artery disease and normal LV function. Biomarkers were negative with an echo showing mild-moderate LVH.
The current ECG showed no new changes, when compared with previous, and serial biomarkers were negative.
READ MORE: Left Ventricular Hypertrophy (LVH) – How to Recognize it on ECG [With Examples]
SIMILAR CASES: