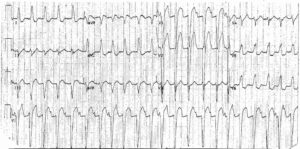
ECG Interpretation
- Sinus tachycardia, rate 125/min
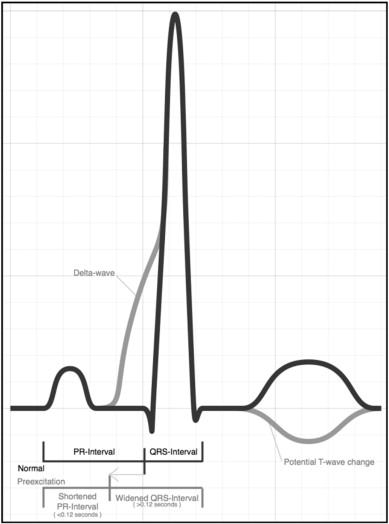
- Short PR interval, most obvious in the chest leads
- Right Axis Deviation (RAD)
- Wide QRS complexes (136 ms)
- Slurred upstroke of the QRS complex (delta wave)
- Dominant R wave in lead V1
- Discordant ST Segment Depression and T wave inversion in Leads V1-4 and inferior leads (II,III,aVF)

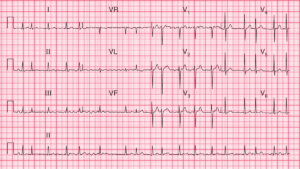
Clinical Interpretation
This ECG is classic of Wolff–Parkinson–White (WPW) syndrome. The resemblance to the ECG of right ventricular hypertrophy (RVH) is because this is WPW type A, with a left-sided accessory pathway.
What to do next?
The patient gives a clear story of a paroxysmal tachycardia, and during attacks he feels dizzy, so the circulation is clearly compromised. The attacks are infrequent, so there is little point in recording an ambulatory ECG.
The patient needs immediate referral to an electrophysiologist for ablation of the aberrant conducting pathway.