ECG Interpretation
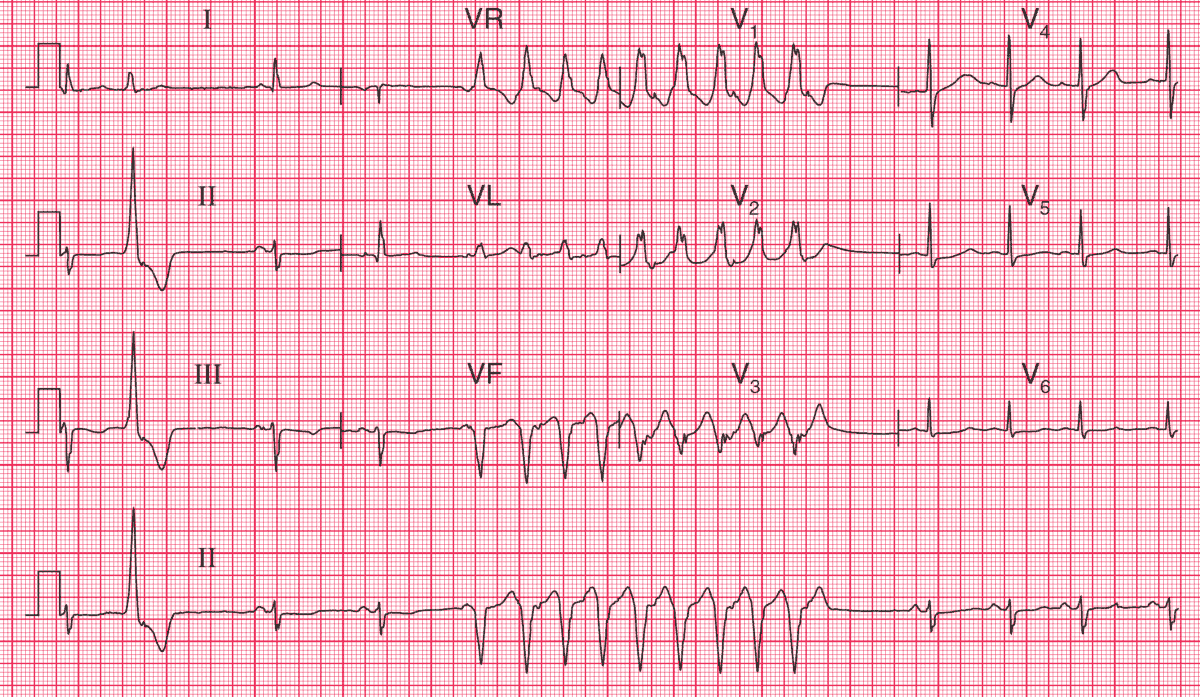
This ECG looks difficult to interpret because there is a nine-beat run of a broad complex tachycardia which occupies the whole of leads V1–V3.
The key is to identify the rhythm first, from the lead II rhythm strip at the bottom. The ECG shows:
- The rhythm is basically sinus, with a rate varying between 65/min and 100/min
- One ventricular extrasystole, at the beginning of the record
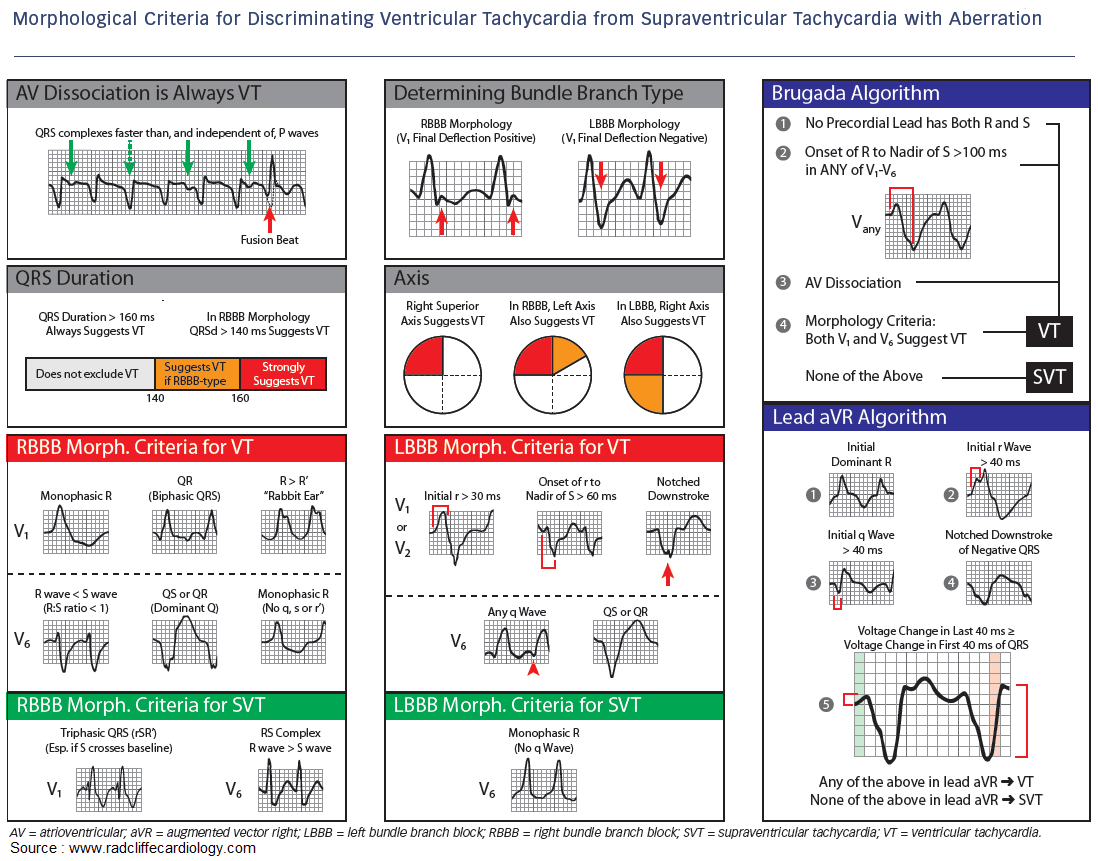
- Broad complex tachycardia with an obviously different morphology from the sinus beats. The QRS complex duration is 160 ms, and in lead V1 the R peak is higher that the R1 peak. These features make it likely that the tachycardia is ventricular in origin
- Left axis deviation in the sinus beats (left anterior hemiblock)
- QRS complexes in the sinus beats otherwise appear normal
- Slight ST segment depression in leads II, III, V5–V6
- T wave inversion in leads II, III
What to do ?
This patient’s attacks of dizziness may be due to the paroxysmal arrhythmia, which is life-threatening. The results of an ambulatory ECG recording and an exercise test would be interesting, but the patient needs immediate treatment, and amiodarone would probably be the drug of choice.
A coronary angiogram should be considered because there may be one or more critical stenoses amenable to percutaneous coronary intervention (PCI), and this might abolish the ventricular tachycardia.
- READ MORE:
- More Similar Cases: