This telemetry strip was recorded during an episode of chest pain. Initially two narrow QRS complexes can be seen (*), both of which are preceded by P waves (+) with a constant PR interval of 0.14 second.
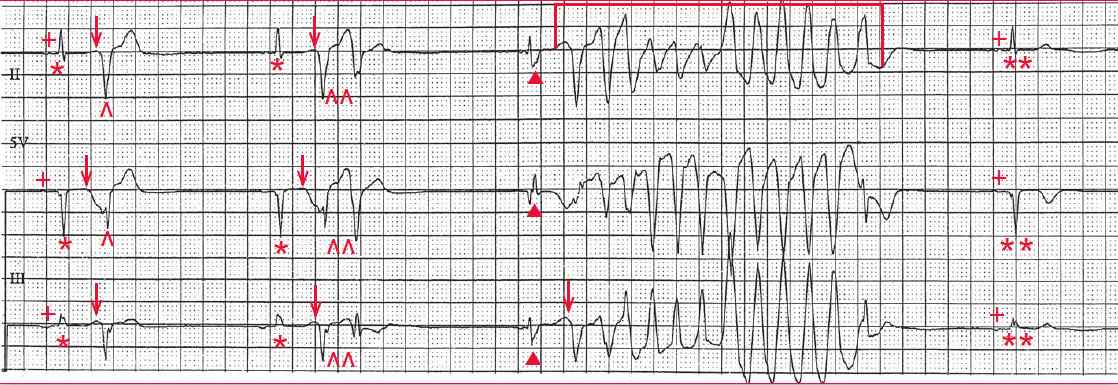
The last QRS complex (**) is also narrow and is preceded by a P wave with the same PR interval (0.14 sec). Importantly, the QT interval is normal (420 msec).
There is a single premature ventricular complex (PVC) (^) after the first narrow QRS complex. The interval between this PVC and the preceding supraventricular complex is short; the PVC occurs slightly after the apex of the T wave, on the early downslope (↓). This is, therefore, an R-on-T PVC.
After the second narrow QRS complex there are two sequential PVCs (^^), termed a ventricular couplet. As before, it is occurring on the downslope of the T wave (↓).
There is a third narrow QRS complex (▲), which is again followed by an R-on-T PVC (↓). However, this PVC provokes a brief episode of polymorphic ventricular tachycardia (┌┐). This tachycardia has QRS complexes that are changing in morphology and axis. Because it is self-terminating, this is termed nonsustained polymorphic ventricular tachycardia.
Polymorphic ventricular tachycardia is seen in two situations and depends on the baseline QT interval. If the QT interval of a sinus or supraventricular complex is normal, it is polymorphic ventricular tachycardia, which is associated primarily with ischemia.
Less commonly seen is polymorphic ventricular tachycardia and a normal QT interval associated with a congenital or familial condition known as catecholaminergic polymorphic ventricular tachycardia. These patients have a structurally normal heart but have a genetic mutation of either a ryanodine or calsequestrin 2 gene.
- READ MORE: ECG Interpretation – All you need to know
- SIMILAR CASES: