
Radiologic Findings
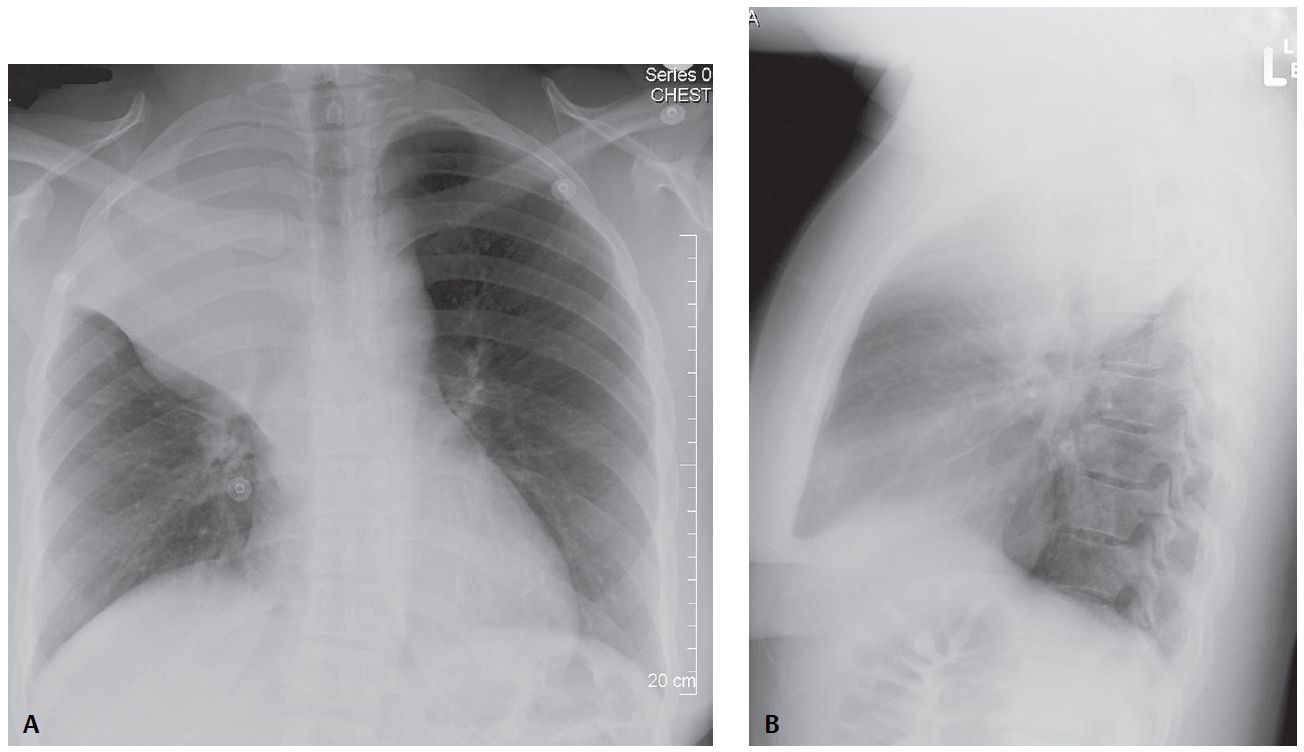
PA and lateral chest X-rays reveal reduction in volume of the right hemithorax, right hemidiaphragm elevation, and a “peaked” appearance (i.e., juxtaphrenic peak) of the superomedial hemidiaphragm. The trachea is minimally displaced to the right.
On the frontal exam, the horizontal fissure is displaced cephalad. A mass-like convex-appearing buge is present in the inferior and medial portion of the fissure. The lateral aspect of the fissure is concave superiorly. The configuration creates a “reverse S shaped” morphology to the fissure.
The lateral exam reveals displacement of both the horizontal and oblique fissures and an indistinct wedge-shaped triangular mediastinal opacity with its apex directed toward the hilum and its base contiguous with the parietal pleura posterior to the apex of the hemithorax.
Diagnosis
Complicated Right Upper Lobe Atelectasis; Lymphoma with “Reverse ‘S’ Sign of Golden”
Differential Diagnosis
- Post-Obstructive Upper Lobe Atelectasis from an Endobronchial Mass (e.g., primary and secondary neoplasia)
- Post-Obstructive Upper Lobe Atelectasis from Extrinsic Bronchial Compression by Reactive or Neoplastic Lymphadenopathy
Background
In non-complicated right upper lobe atelectasis, the inferior border of the horizontal fissure should be concave on frontal and lateral radiography. Complicated right upper lobe atelectasis caused by a hilar mass (e.g., small cell cancer, squamous cell cancer, lymphoma, lymphadenopathy) is often associated with a convex bulge in the medial aspect of the fissure.
The lateral aspect of the fissure is appropriately concave. The result is a “reverse S-shaped” configuration to the horizontal fissure (i.e., reverse “S” sign of Golden), a sign highly suggestive of a central neoplasm causing the atelectasis.
Clinical Findings
Affected patients may present with cough, weight loss, hypoxemia, progressive dyspnea, hemoptysis, diminished or absent breath sounds over the affected area, and various paraneoplastic syndromes.
Imaging Findings
- Opaque right upper thorax
- Direct and indirect signs of right hemithoracic volume loss
- Convex bulge at medial aspect of displaced horizontal fissure
- Central hilar mass lesion or extrinsic bronchial compression by lymphadenopathy
Management
- Prompt bronchoscopic evaluation and biopsy to determine etiology of the complicated lobar atelectasis and establish a tissue diagnosis
- Surgical resection when possible
- Endobronchial stent deployment in select cases
- Palliative chemotherapy and/or radiation therapy in unresectable cases
Prognosis
- Dependent on the stage at presentation in cases of neoplasia
Pearls
- Reverse “S” sign of Golden is highly suggestive of a central bronchogenic cancer as the cause of atelectasis on both radiography and CT. Its presence on chest X-ray should always prompt further investigation with bronchoscopy and/or CT.
- Although initially described for right upper lobe atelectasis, the sign is applicable to atelectasis of any lobe.
- SIMILAR CASES:
Suggested Reading
- Golden R. The effect of bronchostenosis upon the roentgen-ray shadows in carcinoma of the bronchus. Am J Roentgenol 1925;13:21–30
- Proto AV, Tocino I. Radiographic manifestations of lobar collapse. Semin Roentgenol 1980;15(2):117–173
- Reinig JW, Ross P. Computed tomography appearance of Golden’s “S” sign. J Comput Tomogr 1984;8(3):219–223
- Woodring JH, Reed JC. Types and mechanisms of pulmonary atelectasis. J Thorac Imaging 1996;11(2):92–108