This article is an answer to the ECG Case 182
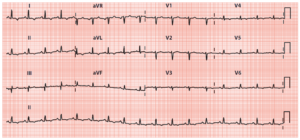
There is a regular rhythm at a rate of 90 bpm. There is a P wave (*) before each QRS complex, with a stable PR interval (0.22 sec). The P wave is upright in leads I, II, aVF, and V4-V6 and negative in lead aVR. This is a normal sinus rhythm with a first-degree AV block.

There are four wide QRS complexes (third, fifth, eighth, and ninth) (+) that are not preceded by a P wave and have an abnormal morphology. These are premature ventricular complexes. In addition, the 15th QRS complex (^) is early. There is a P wave of a different morphology (▼) preceding it, and the QRS complex morphology is the same as the sinus complexes. This is a premature atrial complex. The sinus QRS complex duration is normal (0.10 sec).
There is ST-segment elevation (↓) in leads I, aVL, and V6, and the ST segments have a convex morphology, merging with the T waves. This is an acute lateral wall ST-segment elevation myocardial infarction (STEMI). There is also significant ST-segment depression (↑) in leads II, III, aVF, and V1-V4; these are reciprocal changes.
The premature ventricular complex in leads I and aVL also has ST-segment elevation (▲), indicating that evidence of an acute STEMI can be identified in QRS complexes that are generated by direct activation of the ventricular myocardium, bypassing the normal His-Purkinje pathway (ie, ventricular complexes, paced complexes, or supraventricular complexes with a left bundle branch block). This is based on the Sgarbossa criteria.

MI is quite rare in this age group, raising the possibility of an unusual etiology. MI in the young can be related to:
- vasculitis (such as Kawasaki’s disease)
- chronic inflammatory states
- coronary dissection
- coronary artery embolism from endocarditis or atrial fibrillation
- accelerated atherosclerosis from an inherited dyslipidemia
This young man with a strong family history of coronary disease and physical exam notable for xanthomata likely has an inherited dyslipidemia. The most common of these, familial hypercholesterolemia, is a monogenic, autosomal disorder caused by a defect in the low-density lipoprotein (LDL) receptor.
Patients who harbor the homozygous form of the disease often present with MI during the second or third decade of life. Patients require very aggressive cholesterol-lowering therapy with high-dose statins, inhibitors of cholesterol absorption, and often apheresis.
READ MORE: ECG Interpretation – All you need to know
SIMILAR CASES: