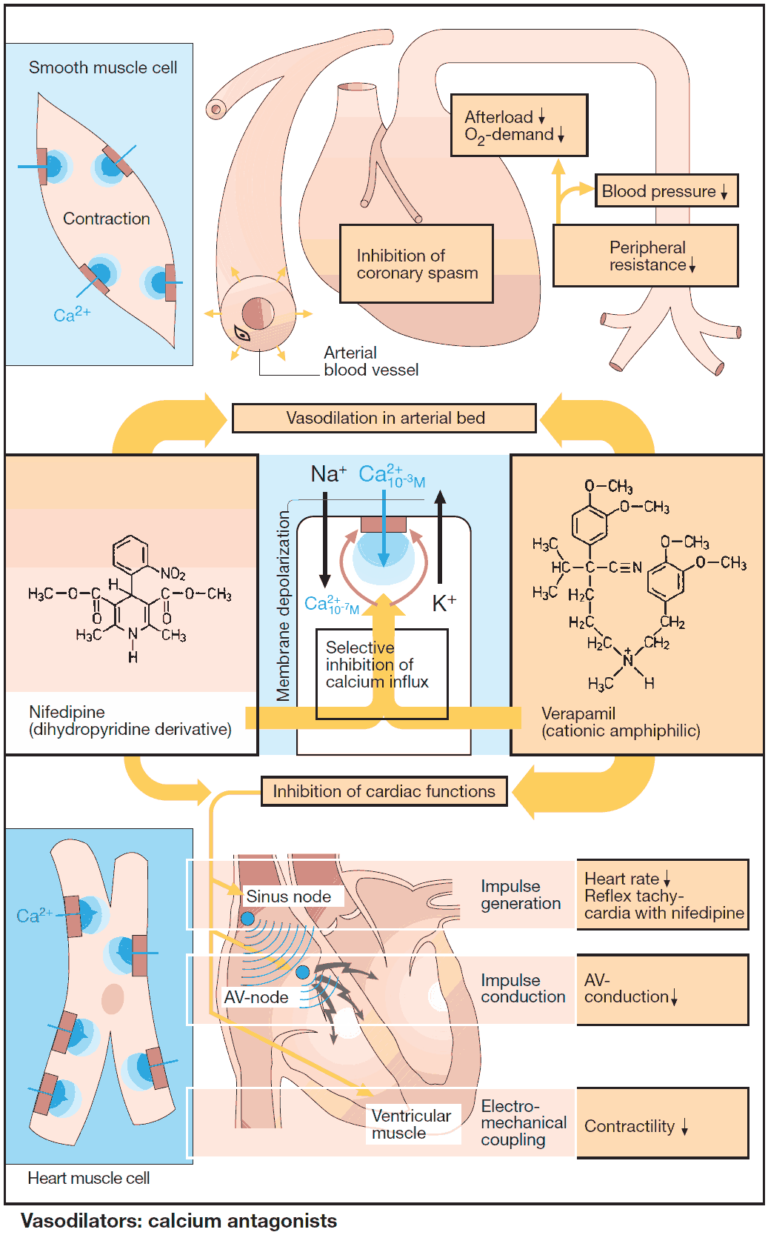
Drugs Acting on Smooth Muscle
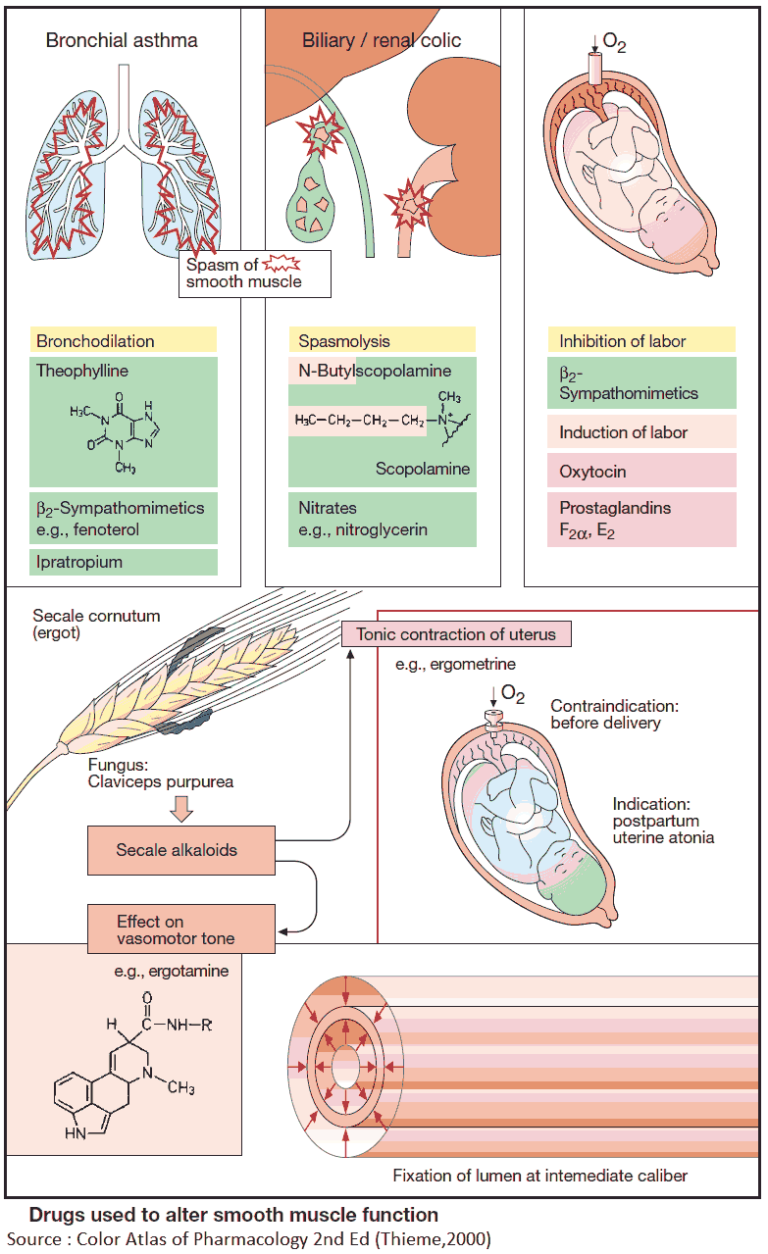
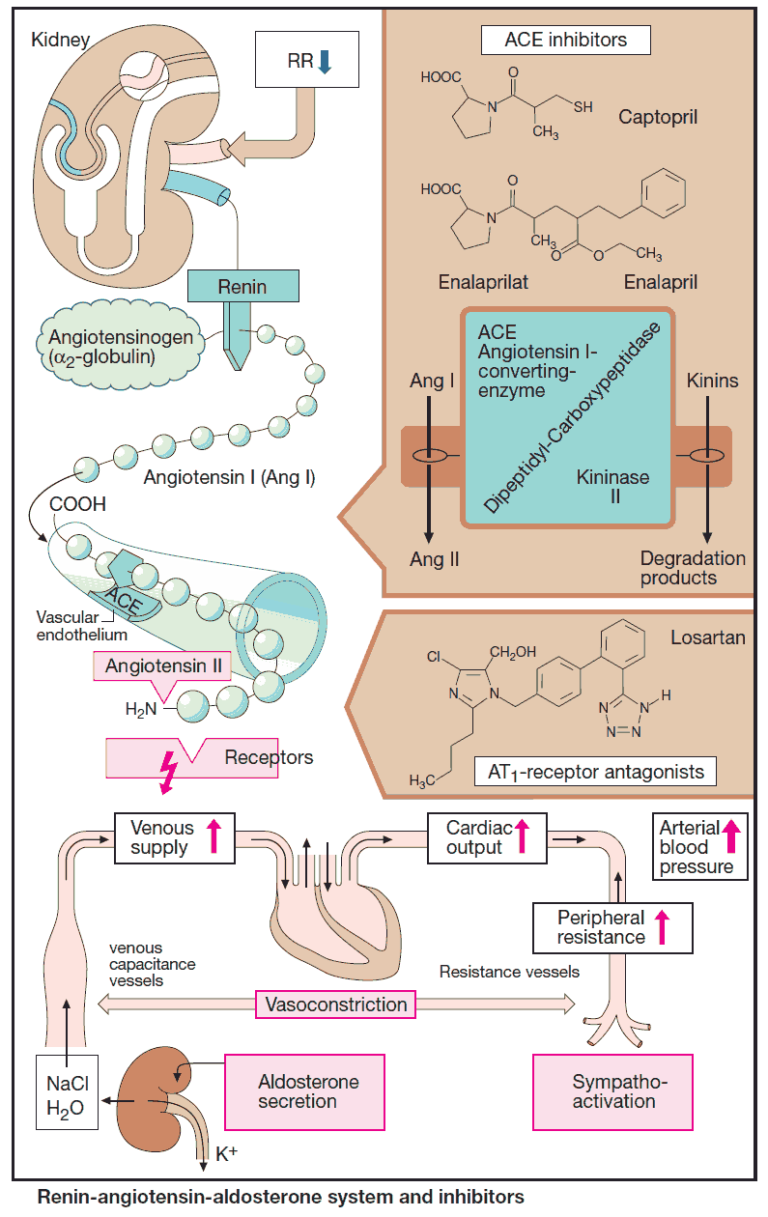
Bronchodilators Narrowing of bronchioles raises airway resistance, e.g., in bronchial or bronchitic asthma. Several substances that are employed as bronchodilators are: β2-sympathomimetics (given by pulmonary, parenteral, or oral route)methylxanthine theophylline…