This article is an answer to the Case – An 8-year-old Girl with Light Cough when Laying Down
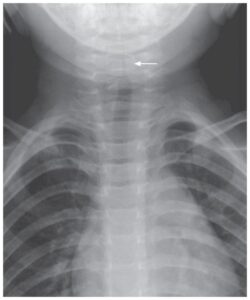
Posteroanterior chest radiograph showed a rounded solid mass in the right cardiophrenic angle. The mass was heterogeneous but it had well-defined border. Pulsed fluoroscopy revealed the presence of large colon within the anterior right hemithorax with peristalsis present.
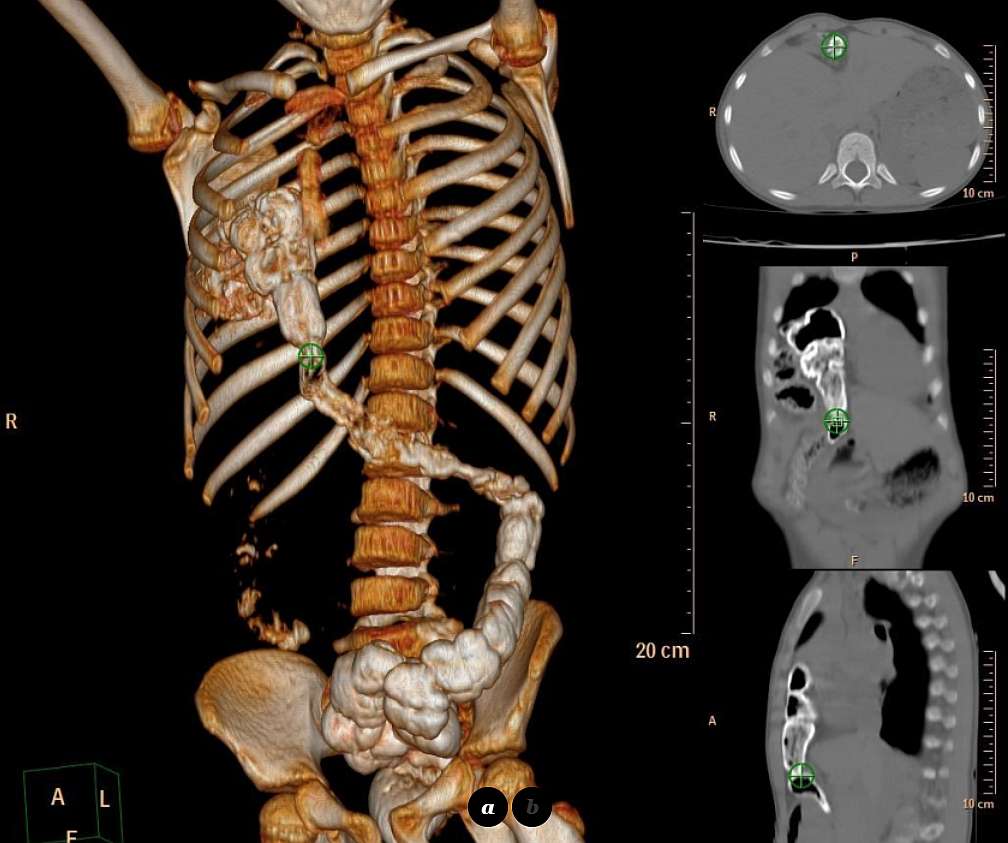
Computed tomography (CT) with multiplanar reconstruction (MPR), performed the following day showed a multilobulated heterogenous mass, with 9 cm at its maximal diameter, showing a regular thin border and entering (from the abdomen) the anterior and medial right hemithorax.
The mass was filled with oral contrast medium taken one day before, and lot of free air was shown within it as well. The hepatic flexure and most part of transverse colon – non-incarcerated – was herniated through the Morgagni foramen (image below). The diagnosis was confirmed surgically a few days later during surgical repair of the congenital defect.
Discussion
Intrathoracic herniation of abdominal contents occurs through congenital defects in the muscle, through traumatic tears or, most commonly, through acquired areas of weakness at the central oesophageal hiatus. Bochdalek and Morgagni hernia are the most frequently occurring congenital herniations of the diaphragm.
Bochdalek hernias are located posterolaterally and are more frequent (9: 1) than the anteromedially located Morgagni hernias [1]. They are more frequently located on the left than on the right side (5:1). They are found in small children and usually contain retroperitoneal fat or a portion of kidney or spleen [2].
Morgagni hernias are due to an anteromedial diaphragmatic defect caused by maldevelopment of the transverse septum. Morgagni hernias are more frequent on the right than on the left (5: 1). They are seen in older children or adults and are usually small. These hernias frequently contain omentum and may contain gut. The incidence of Morgagni hernia detected in the neonatal period because of symptoms is low. In older children and adults, Morgagni hernia is often an incidental finding. Although the weak area at the fibrotendinous elements between the costal and the crural part of the diaphragm is congenital, Morgagni hernia can be acquired. Increase in abdominal pressure due to severe effort, trauma or obesity is probably responsible [3-6].
A Morgagni hernia presents in older children and adulthood as an anterior opacity at the right cardiophrenic angle. It frequently contains omentum and may contain gut. Its smooth, well-defined margin and soft tissue radiodensity usually allows its differentiation from the much more common fat pad collection at this site. It is more difficult to differentiate from a low-lying pericardial cyst.
When bowel is herniated to the chest, the diagnosis can usually be made with conventional chest plain film and barium studies. But the diagnosis is more simply established by means of computed tomography (CT) which can identify diaphragmatic defect especially using MPR and it can also be helpful in determining the nature, relationship of the herniated organs, the precise side and size of the diaphragmatic defect in patients with non-traumatic acquired defects.
CT-MPR is useful for the differential diagnosis with hiatal hernia, pericardial cyst, hemidiphragmatic bulging, cystic masses of lung or mediastinum, oesophageal diverticule etc, as well. Treatment of Morgagni hernia is reponation of the herniated material and diaphragmatic repair in surgery [6-10].
Differential Diagnosis
- Transverse colon herniated through Morgagni foramen
- Hiatal hernia
- Pericardial cyst
- Anterior madiastinal masses
- Cystic masses of lung
SIMILAR CASES:
References
- [1] Snyder WH, Greany EM (1965) Congenital diaphragmatic hernia; 77 consecutive cases. Surgery 57:576–588 (PMID: 14275786)
- Gale ME (1985) Bochdalek hernia: prevalence and CT characteristics. Radiology 156:449–452 (PMID: 4011909)
- Paris F, Tarazona V, Casillas M et al (1985) Hernia of Morgagni. Thorax 28:631 (PMID: 4784388)
- Lojszczyk-szczepaniak A, Komsta R, Debiak P (2011) Retrosternal (Morgagni) diaphragmatic hernia. Can. Vet. J 52 (8): 878-83 (PMID: 22294795)
- El-sharkawy A, Higashi Y, Lobo D (2012) Education and imaging. Gastrointestinal: foramen of Morgagni hernia in an adult. J. Gastroenterol. Hepatol 27 (3): 616 (PMID: 22353349)
- Eren S, Ciri F (2005) Diaphragmatic hernia: diagnostic approaches with review of the literature. Eur J Radiol 54:448–59 (PMID: 15899350)
- Pokorny CW, McGill, Harberg FJ (1984) Presentation of Morgagni hernias during infancy: Presentation and associated anomalies. J Pediatr Surg 19:394 (PMID: 6481584)
- Coulier B, Ramboux A, Mailleux P et al (1999) Diagnosis of non-hiatal diaphragmatic hernia using helical computed tomography. JBR BTR 82:1–5 (PMID: 11155856)
- Gale ME (1986) Anterior diaphragm: variations in the CT appearance. Radiology 161:635–639 (PMID: 3786709)
- Loong TP, Kocher HM (2005) Clinical presentation and operative repair of hernia of Morgagni. Postgrad Med J 81:41–4 (PMID: 15640427)