Table of Contents
Resuscitation and Critical Diagnosis
General
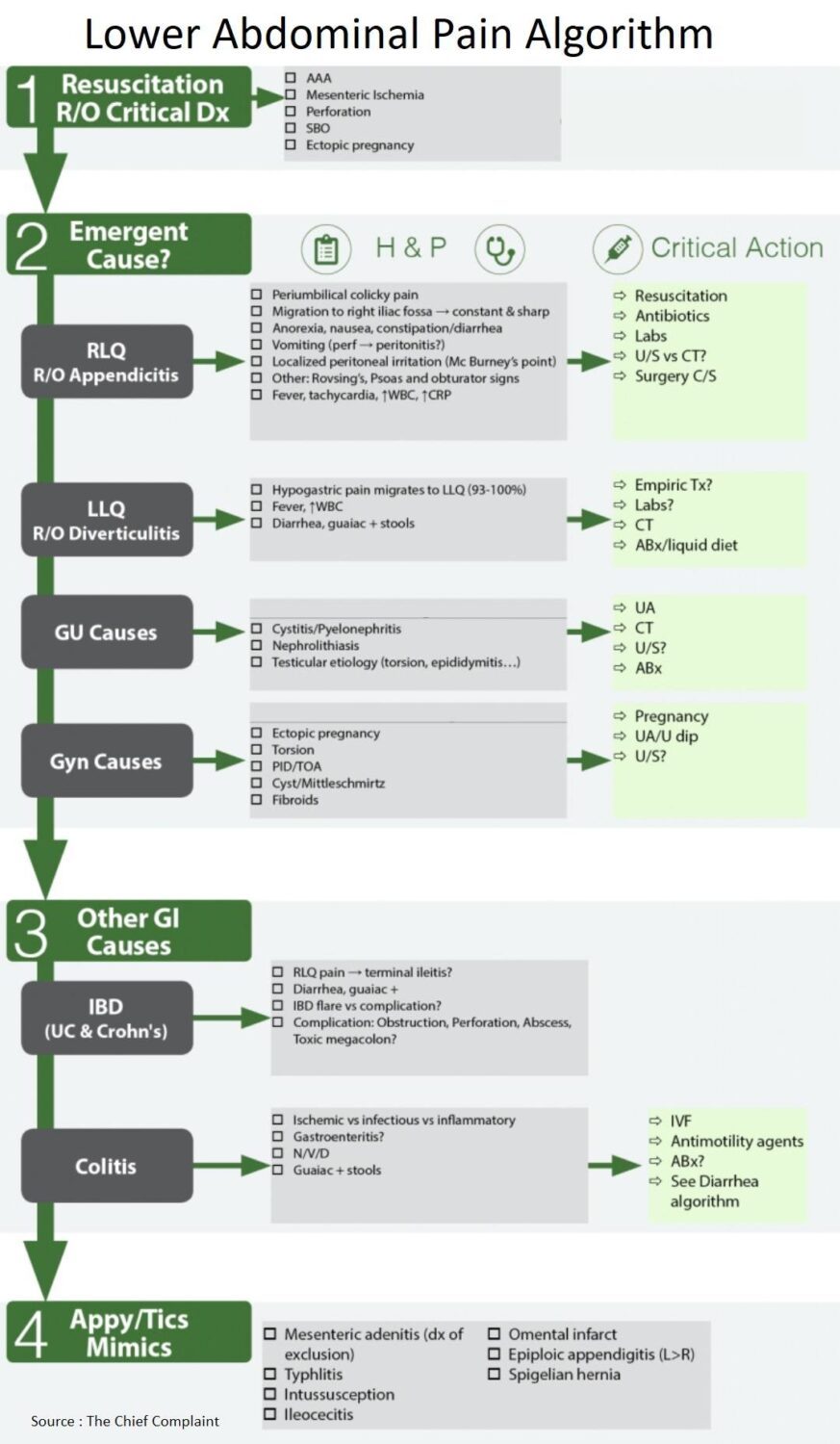
- Work-up for lower abdominal pain begins with resuscitation and exclusion of critical diagnoses
- AAA (Abdominal Aortic Aneurysm)
- Mesenteric Ischemia
- Perforation
- SBO (small bowel obstruction)
- ectopic pregnancy
- Then, through a detailed history and physical, consider all the causes of lower abdominal pain
- Rule out Genitourinary causes (pyelonephritis vs kidney stone) if possible with Urine Analysis
- The differential may then come down to GI (appendicitis, diverticulitis) vs pelvic etiology (in females) → will need further imaging based on suspicion (CT A/P vs pelvic ultrasound)
Resuscitate
• IV/O2/Monitor, IV Fluids, Labs as needed, pregnancy test
Rule Out Critical diagnoses:
• AAA, Mesenteric Ischemia, Perforation, SBO, ectopic pregnancy

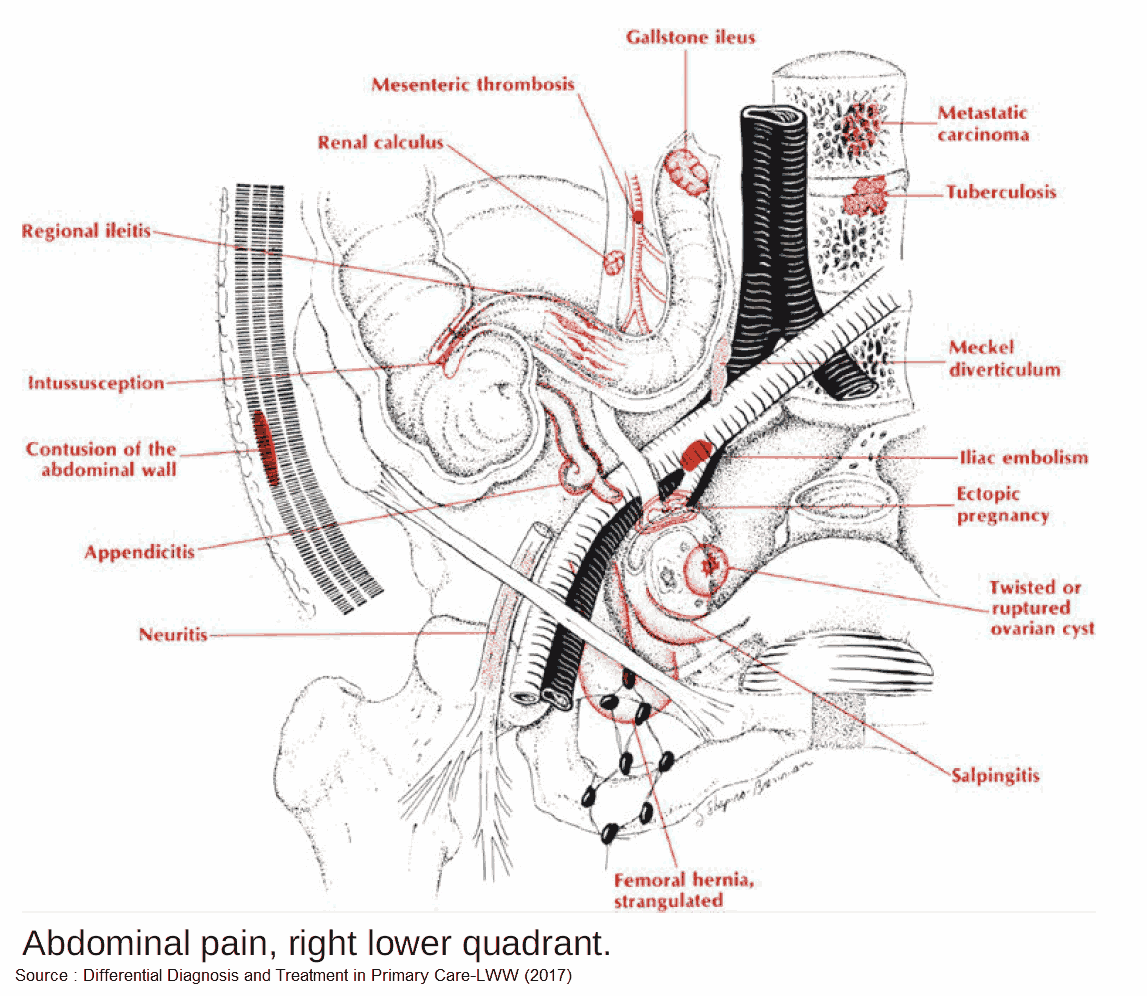
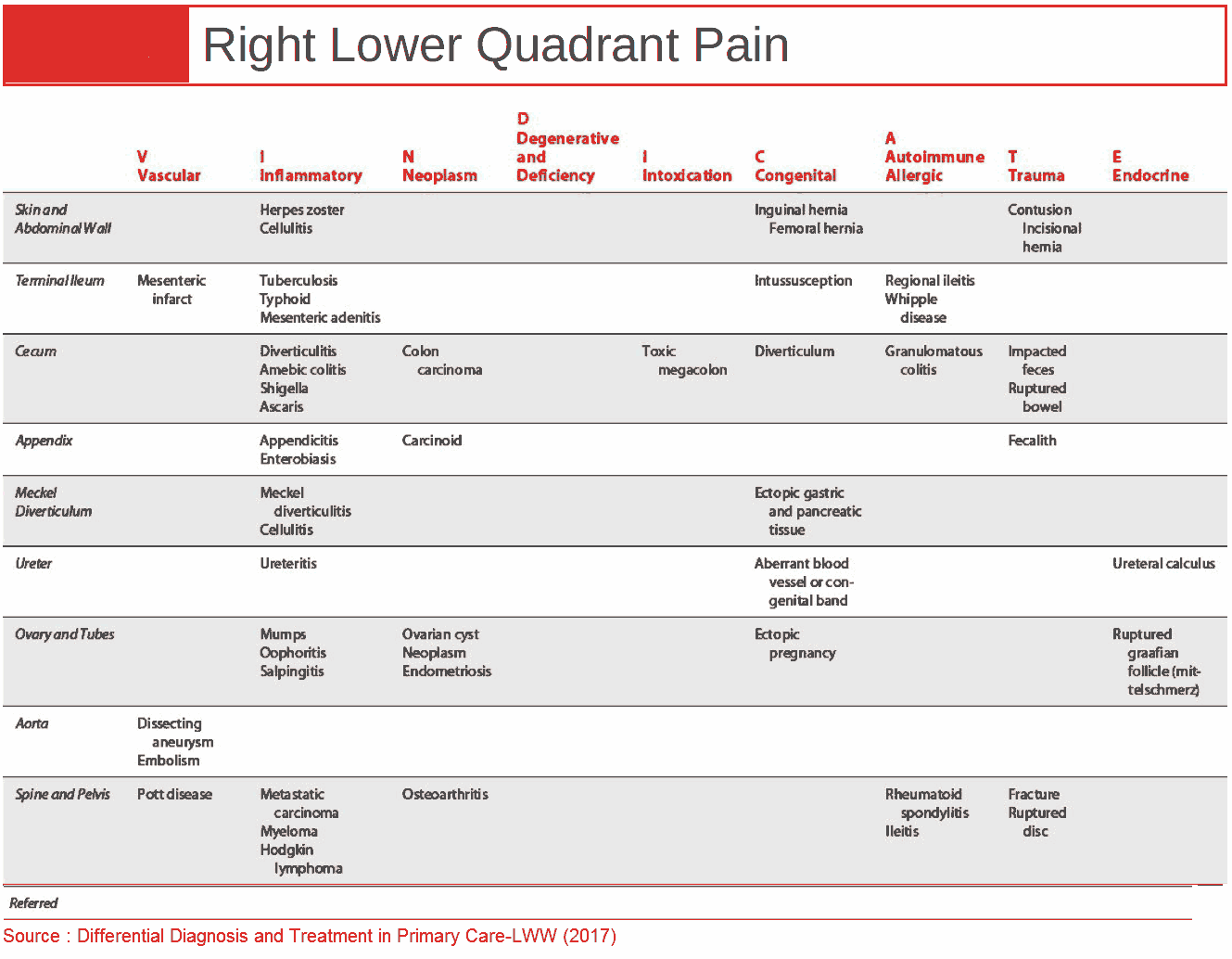
Differential Diagnosis for Abdominal Right Lower Quadrant (RLQ) Pain 
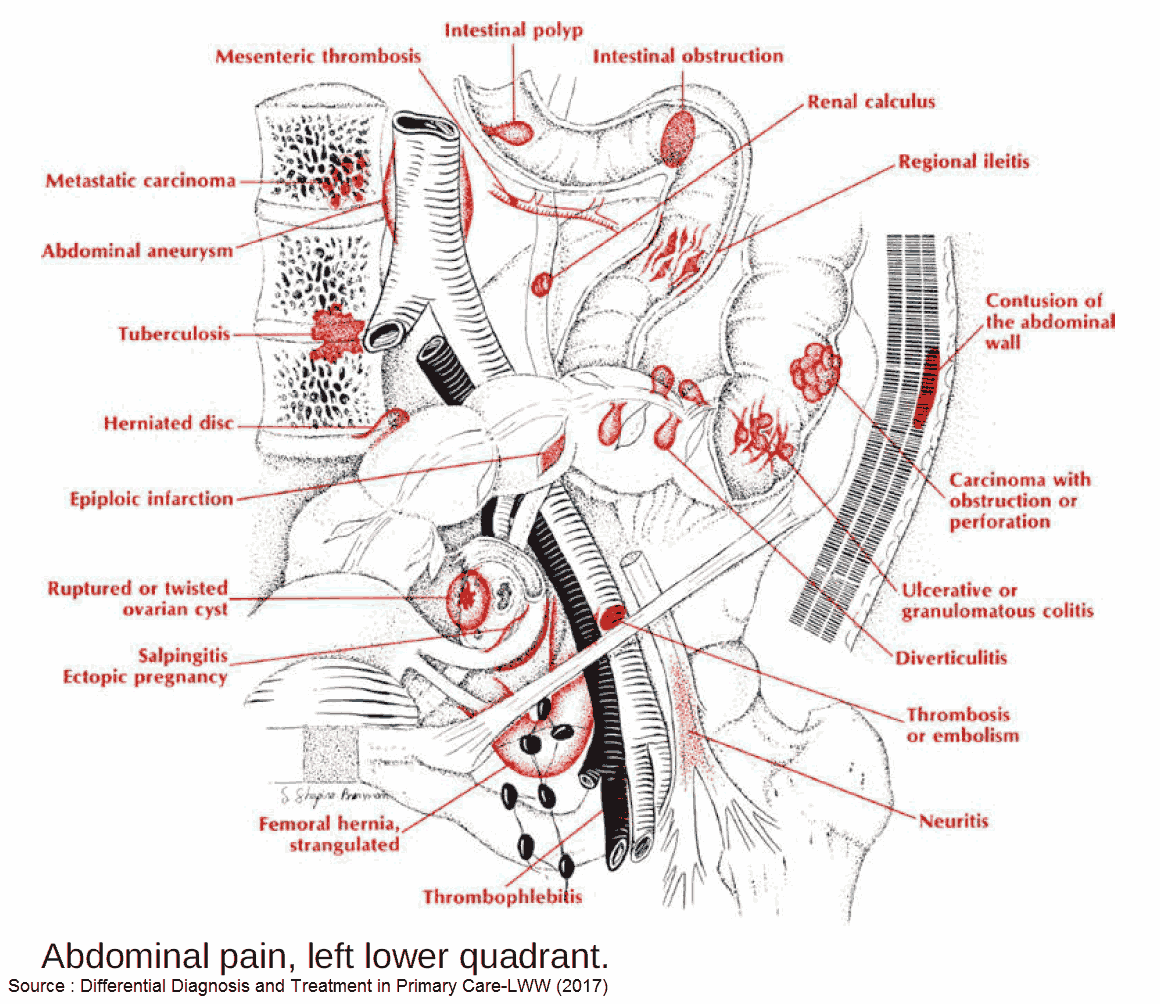
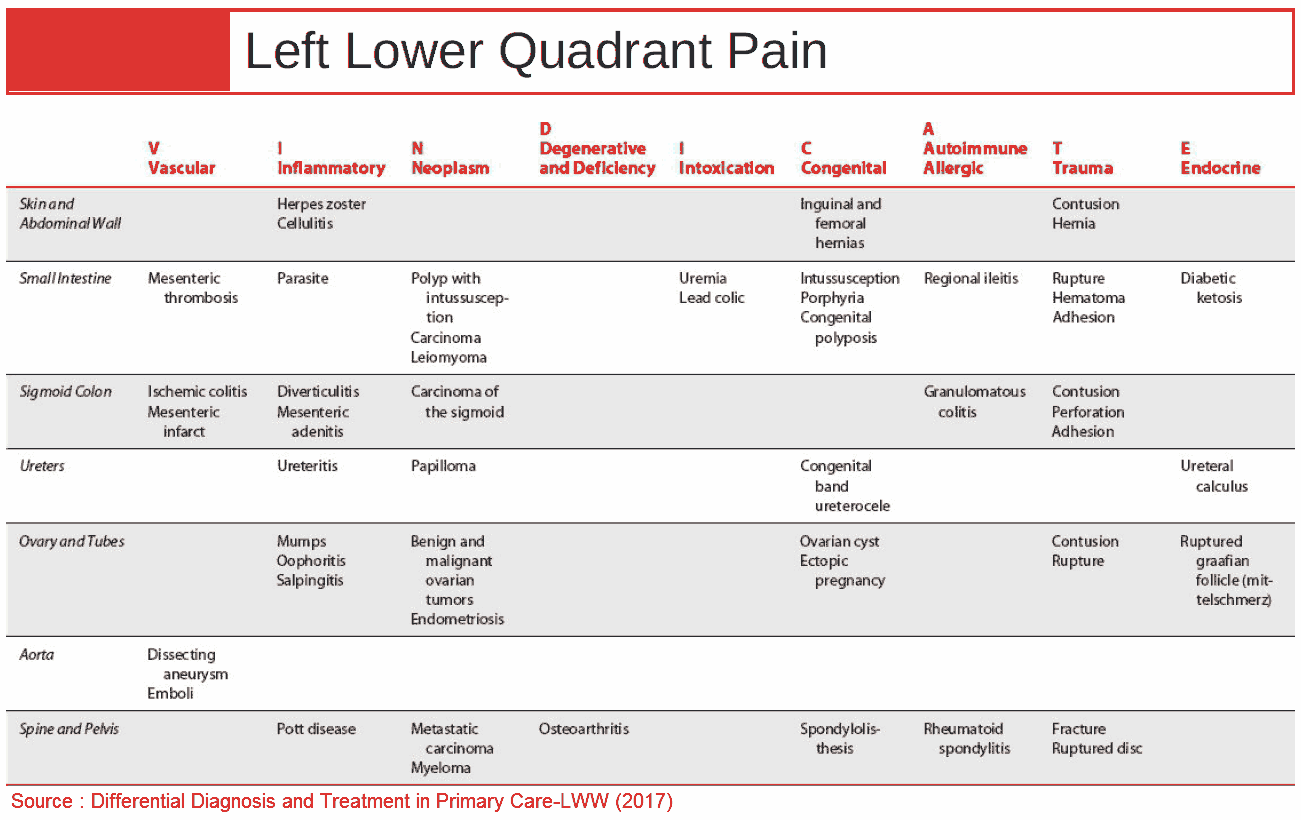
Differential Diagnosis for Abdominal Left Lower Quadrant (LLQ) Pain 
Abdominal Right Lower Quadrant Pain 
Abdominal Left Lower Quadrant Pain
Emergent Causes of Lower Abdominal Pain
1. Appendicitis
Clinical Presentation of Appendicitis
- General
- Abdominal pain
- Periumbilical colicky pain
- Migration to right iliac fossa → constant and sharp
- Localized peritoneal irritation (McBurney’s point)
- Rovsing’s (palpation in LLQ elicits pain in RLQ)
- Psoas (passive extension of thigh or active flexion of hip → pain → retrocecal appendicitis)
- Obturator signs (flexion and internal rotation of hip → pain)
- Anorexia, nausea / vomiting, constipation / diarrhea
- Fever, tachycardia, High WBC, High CRP
- Abdominal pain
- Strongest predictors of appendicitis (Meta-analysis Brit J Surg 2004;91:28-37)
- Inflammatory response variables (PMN, WBC, CRP)
- Peritoneal irritation (rebound, percussion tenderness, guarding, rigidity)
- Migration of pain (epigastric/periumbilical → RLQ (right lower quadrant))
- Patients at extremes of age may have non-specific symptoms → diagnostic difficulty
Appendicitis Triad
□ Inflammatory markers
□ Peritoneal irritation
□ Migration of pain
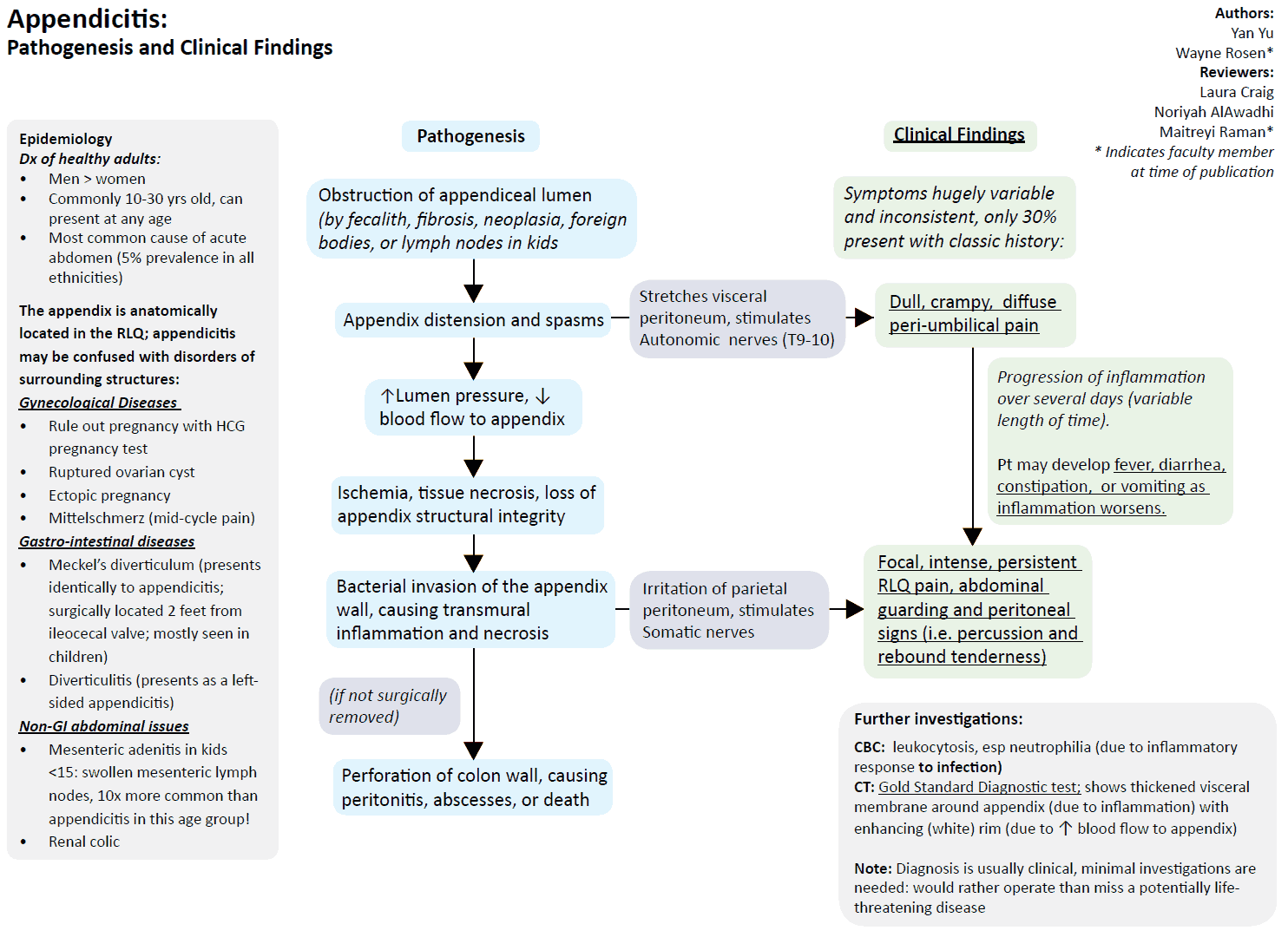
Work-up for Appendicitis (Ann Intern Med 2004;141:537-46)
- Ultrasound
- Aperistaltic and non-compressible structure > 6mm
- Sensitivity 86%; Specificity 81%
- CT
- Abnormal appendix, calcified appendicolith + periappendiceal inflammation or diameter >6mm
- Sensitivity 94%; Specificity 95%
Treatment of Appendicitis
- Resuscitation
- Large bore IV, IV Fluids
- Pain control
- Opiate administration has no significant association with management errors (JAMA 2006;296:1764-1774)
- Antibiotics
- Broad spectrum, empiric
- Lower Incidence of postoperative wound infection and intra-abdominal abscess formation (Cochrane Database Syst Rev 2005;(3):CD001439)
- Antibiotics alone for treatment? (Lancet. 2011:377(9777):1573)
- Spontaneous resolution can also occur
- 1 year recurrence rate with antibiotics as sole therapy → 15% most within 10 days
- Surgery
- Risk of rupture: 0-36h → <2%;
- Each ensuing 12h period after 36h → 5%
- Timing (Arch Surg 2006;141:504-7)
- No significant difference between early (<12h after presentation) and later (12- 24h) appendectomy
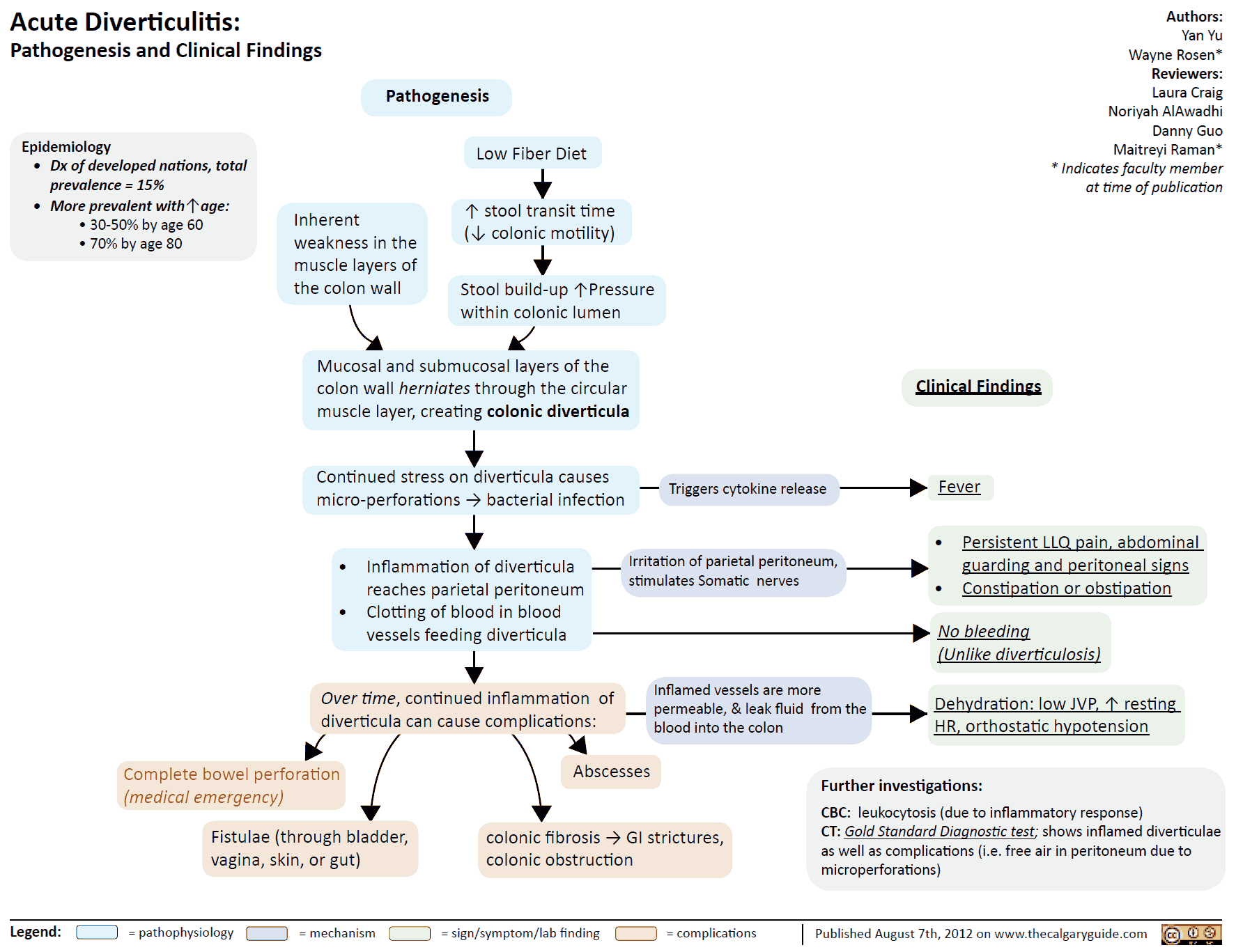
2. Diverticulitis
Clinical Presentation
- Presents like appendicitis, but of the LLQ (lower left quadrant)
- Hypogastric pain migrates to LLQ (93-100%)
- Fever, High WBC
- Diarrhea, guaiac + stools
Work-up for Diverticulitis (Am J Roentgenol 2002;178:1313-8)
- Empiric treatment ?
- No imaging studies needed if diagnosis is clear-cut → can begin empiric treatment
- CT
- Sensitivity 69-95%, Specificity 75-100%
- Use for uncertain diagnosis, exclude other causes of abdominal pain, rule out diverticular complications, or clinical deterioration
- Findings: bowel wall thickening (96%), fat stranding (95%), detects complications (free air, abscess, phlegmons, cancer)
- Ultrasound
- Sensitivity 84%, Specificity 93%
- Rule out AAA, hypoechoic bowel wall thickening, diverticula, abscess, hypoechoic around bowel wall
Complications of Diverticulitis (Emerg Med Clin N Am 2003;21:937-969)
- Abscess
- Can lead to fistula formation, sepsis
- Free perforation, peritonitis
- Rupture of diverticular abscess → acute surgical abdomen
- More common In elderly and immunosuppressed, high mortality (6-25%)
- Fistula
- Fistula between colon and surrounding structures → colovesicular, colovaginal, colocutaneous, coloenteric
- Colovesicular most common (dysuria, pyuria, pneumaturia, fecaluria)
- Obstruction
- Uncommon-2% of cases
- May cause Small-Bowel Obstruction when loops of bowel entangled in peridiverticular adhesions
Treatment of Diverticulitis
- Outpatient
- Indication: Mild symptoms, tolerating oral fluids, well appearing (Am Fam Physician 2005;72(7):1229)
- Antibiotics, 7-10days (Amoxicillin / Clavulanic acid, TMP/SMX (Trimethoprim / Sulfamethoxazole), ciprofloxacin/metronidazole)
- Liquid diet, may consider no antibiotics in extremely well appearing pts (Br J Surg 2012;99(4):532)
- If no improvement in 2-3 days → consider peridiverticular disease (reassessment and admission?)
- Inpatient
- Indication: Severe symptoms requiring narcotics, unable to tolerate oral fluids, elderly, comorbid illnesses, ill/septic, no home support or follow-up
- IV antibiotics (gram negative/anaerobes), bowel rest
- Laparotomy? → generalized peritonitis, sepsis, visceral perforation, clinical deterioration
3. Pyelonephritis
4. Nephrolithiasis
5. Torsion / PID / TOA
6. Acute Scrotum
Other Causes of Lower Abdominal Pain
1. IBD (Inflammatory bowel disease)
Clinical Presentation
- RLQ pain → terminal ileitis ?
- Diffuse abdominal pain, diarrhea, guaiac +
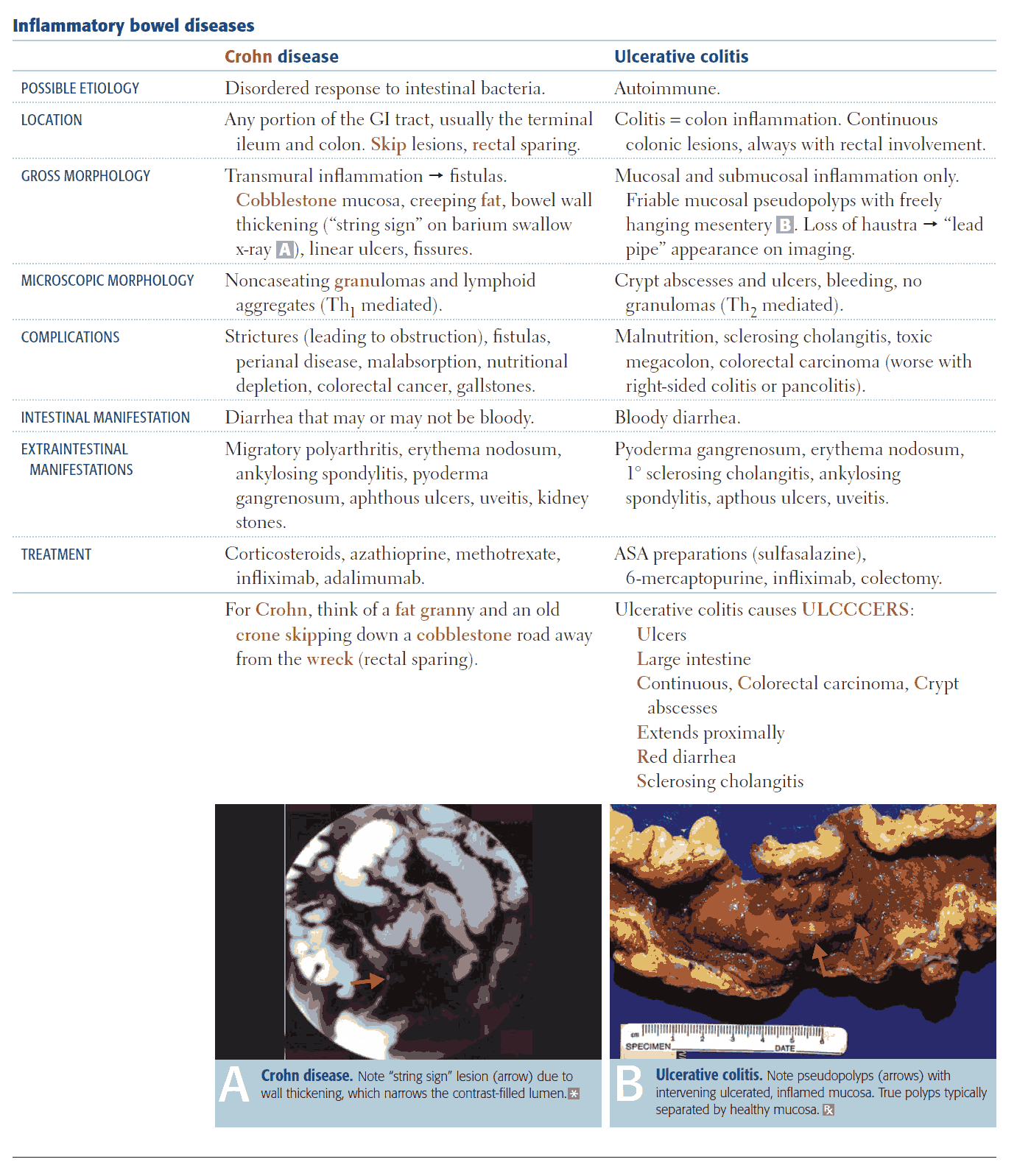
Complications
- May be difficult to distinguish “flare” from an acute complication → consider further diagnostic imaging
- TOXIC MEGACOLON
- Define: Lethal complication of IBD or infectious colitis → total or segmental nonobstructive colonic dilatation plus systemic toxicity
- Clinical: abrupt onset bloody diarrhea, fever, High WBC, tachycardia, third space losses, ill appearing, abdominal distension → perforation (peritoneal signs may be masked by steroids)
- Therapy: Resuscitation, blood transfusion, broad spectrum antibiotics, corticosteroids, +/- immunosuppressants, bowel rest and bowel decompression
- Surgery: indicated if no improvement on medical therapy (subtotal colectomy with endileostomy)
- Hemorrhage: (CD > UC) → Resuscitation, blood transfusion, surgery consult (bowel resection?)
- Other: Obstruction, Perforation, Abscess
2. Colitis
- Etiology
- Ischemic vs infectious vs inflammatory
- Mesenteric Ischemia
- Clinical Presentation
- Gastroenteritis ?
- N/V/D
- Guaiac + stools
Other Appendicitis Mimics
- Mesenteric adenitis (diagnosis of exclusion)
- Typhlitis
- Intussusception
- Ileocecitis
- Omental infarct
- Epiploic appendigitis (L>R)
- Spigelian hernia
References
- https://www.bmj.com/content/333/7567/530
- https://pubmed.ncbi.nlm.nih.gov/20116016/
- https://pubmed.ncbi.nlm.nih.gov/14716790/
- https://pubmed.ncbi.nlm.nih.gov/15466771/
- https://jamanetwork.com/journals/jama/article-abstract/203613
- https://pubmed.ncbi.nlm.nih.gov/16034862/
- https://pubmed.ncbi.nlm.nih.gov/21550483/
- https://jamanetwork.com/journals/jamasurgery/article-abstract/398369
- https://pubmed.ncbi.nlm.nih.gov/12034590/
- https://pubmed.ncbi.nlm.nih.gov/14708814/
- https://pubmed.ncbi.nlm.nih.gov/16225025/
- https://pubmed.ncbi.nlm.nih.gov/22396052/