ECG Interpretation
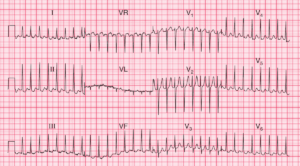
- Atrial fibrillation, ventricular rate about 100/min, with one ventricular extrasystole
- Normal axis
- Broad QRS complexes, with morphology of left bundle branch block (LBBB)
- T waves inverted in lateral leads, as expected in LBBB
The chest X-ray showed a very large heart, all chambers being affected.
What to do ?
This patient has had no chest pain, but has developed a very large heart with atrial fibrillation; the ECG shows LBBB. Ischaemia seems unlikely, and the diagnosis is almost certainly dilated cardiomyopathy of unknown cause.
An echocardiogram may show some mitral regurgitation due to left ventricular dilatation, but the valves will probably be structurally normal. There will probably be globally reduced left ventricular function with a low ejection fraction.
It is unlikely that a primary cause will be found, though alcoholism is the important one to exclude.
A coronary angiogram should probably be performed to exclude ‘silent’ coronary disease, and an endomyocardial biopsy could be considered, to exclude the remote chance of a primary cardiomyopathy.
Treatment would be the usual combination of diuretics, an angiotensin-converting enzyme inhibitor, digoxin, anticoagulants and ultimately cardiac transplantation.
- READ MORE:
- Similar Cases:
- Atrial Fibrillation with Rate Related RBBB
- Atrial Fibrillation and LBBB
- ECG Case 85: Posterior MI and Atrial Fibrillation
- ECG Case 80: Atrial Fibrillation and WPW Syndrome
- ECG Case 71: Atrial fibrillation with RVR, LAFB and Acute Anterolateral STEMI
- ECG Case 66: Atrial Fibrillation with an Uncontrolled Ventricular Rate